See: Sialograms and Sialography
30 Second Sialography Video (Condensed 18x speed - silent):
9 Minute Sialography Instruction Video (Annotated with Sound):
(suggest click off the cc: to avoid duplicate annotation)
Background:
A recent (August 2025) publication through a contemporary assessment of a series of diagnostic submandibular sialograms concluded that sialography "is often therapeutic and is performed with limited radiation exposure" (Molotkova 2025).
Case #1 Radioiodine (Parotid Glands)
Presentation: 36 yo with 6 months of recurrent bilateral parotid swelling and pain with onset of dry mouth beginning 6 months after receiving 156 mCi radioiodine 1 year ago. Pain with and without meals.
Exam: soft parotid glands with dry mouth unable to produce saliva with massage of glands
CT: unremarkable salivary glands
Ultrasound (POCUS at time of visit):

Panel Discussion Regarding Management
Outcome: Case #1 Parotid Swelling and Pain with Xerostomia after Radioiodine
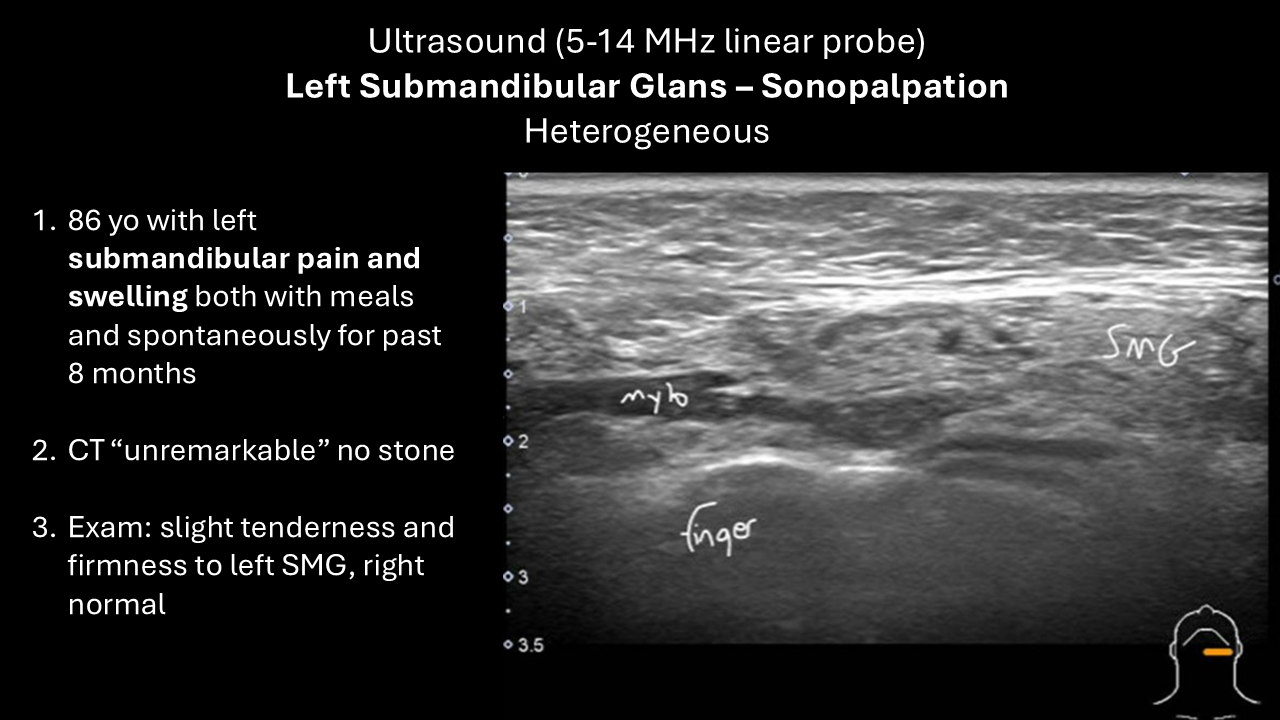
Case #2 Sialadenitis (Submandibular)
Presentation: 86 yo with left submandibular pain and swelling both with meals and spontaneously over 8 months.
Exam: slight tenderness and firmness to left submandibular gland, right is normal
CT: unremarkable salivary glands - no stone
Ultrasound (POCUS at time of visit):
Panel Discussion Regarding Management
Outcome: Case # 2 Submandibular Gland Swelling and Pain
Case #3 Sjogren's Syndrome (Parotid Swelling and Pain)
Presentation: 56 yo with 30+ yrs of xerostomia and xeropthalmia dx Sjogrens 15 yrs ago with +SSA +SSB. Has bilateral parotid swelling and pain every 4 weeks. Massage causes nasty taste in mouth
Exam: unremarkable (currently nontender) parotid glands with dry mouth unable to produce saliva with massage of glands
CT: atrophy of smg's; parotid glands with areas of fatty infiltration
Ultrasound (POCUS at time of visit):
Panel Discussion Regarding Management
Outcome: Case #3 Sjogren's Syndrome (Parotid Swelling and Pain)
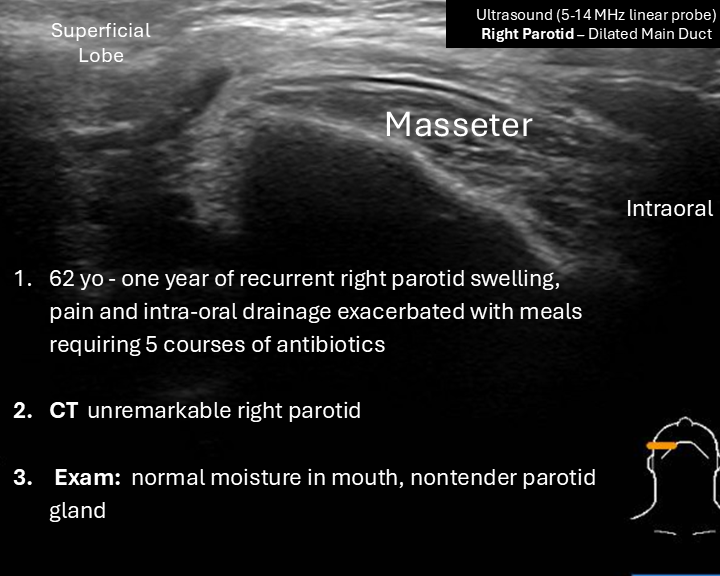
Case #4 Right Parotid Recurrent Sialadenitis
Presentation: 62 yo with one year history of recurrent right parotid swelling and pain with intermittent intraoral drainage exacerbated by meals requiring 5 courses of antibiotics to resolve
Exam: Soft nontender right parotid - intraoral unremarkable; s/p left parotidectomy for tumor
CT: unremarkable
Ultrasound (POCUS):
Panel Discussion Regarding Management
Outcome: Case #4 Right Parotid Sialadenitis
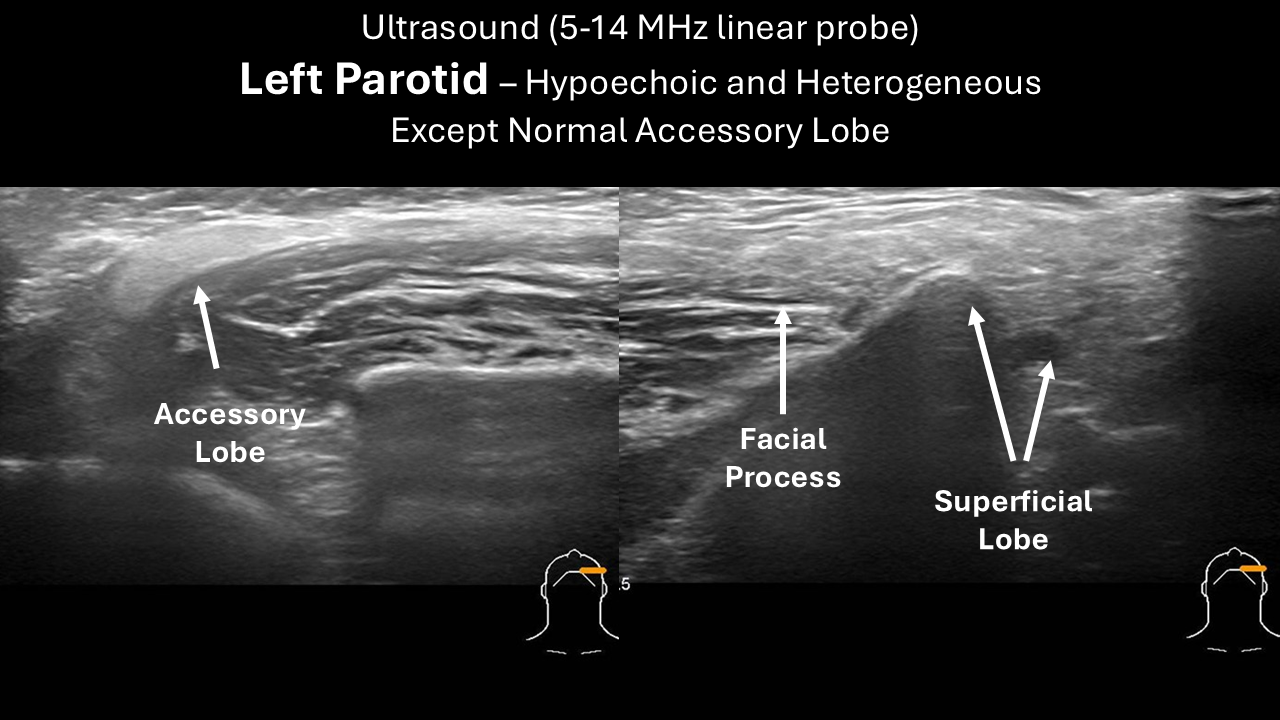
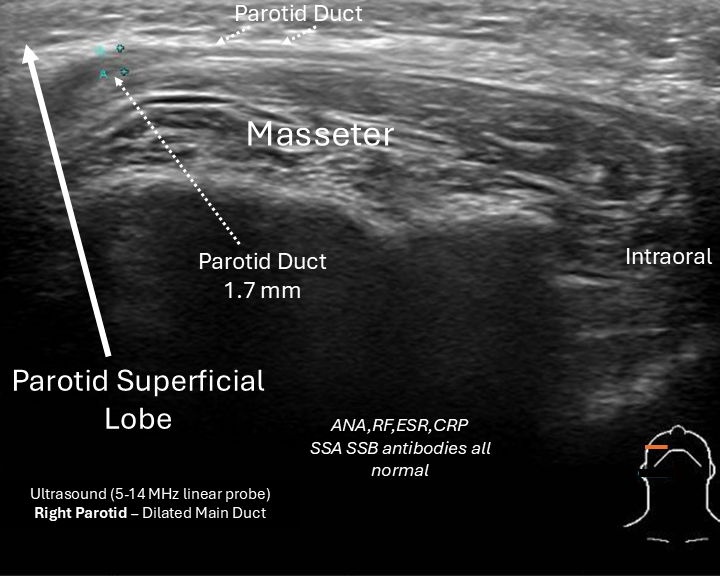
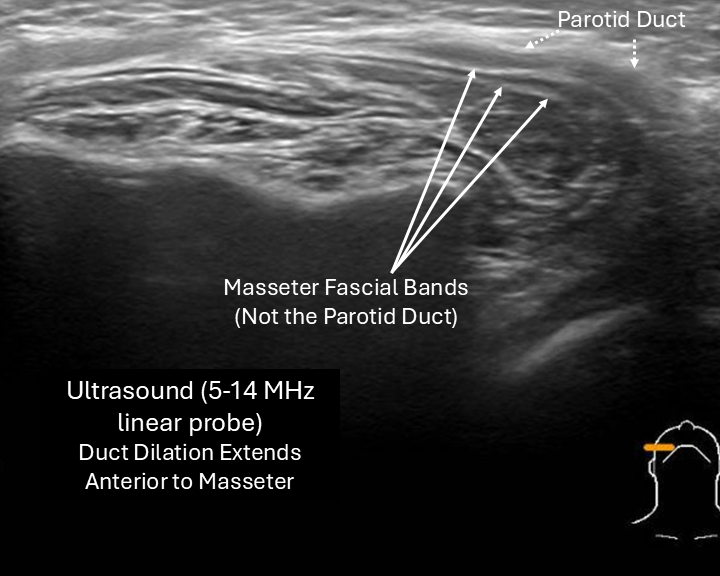
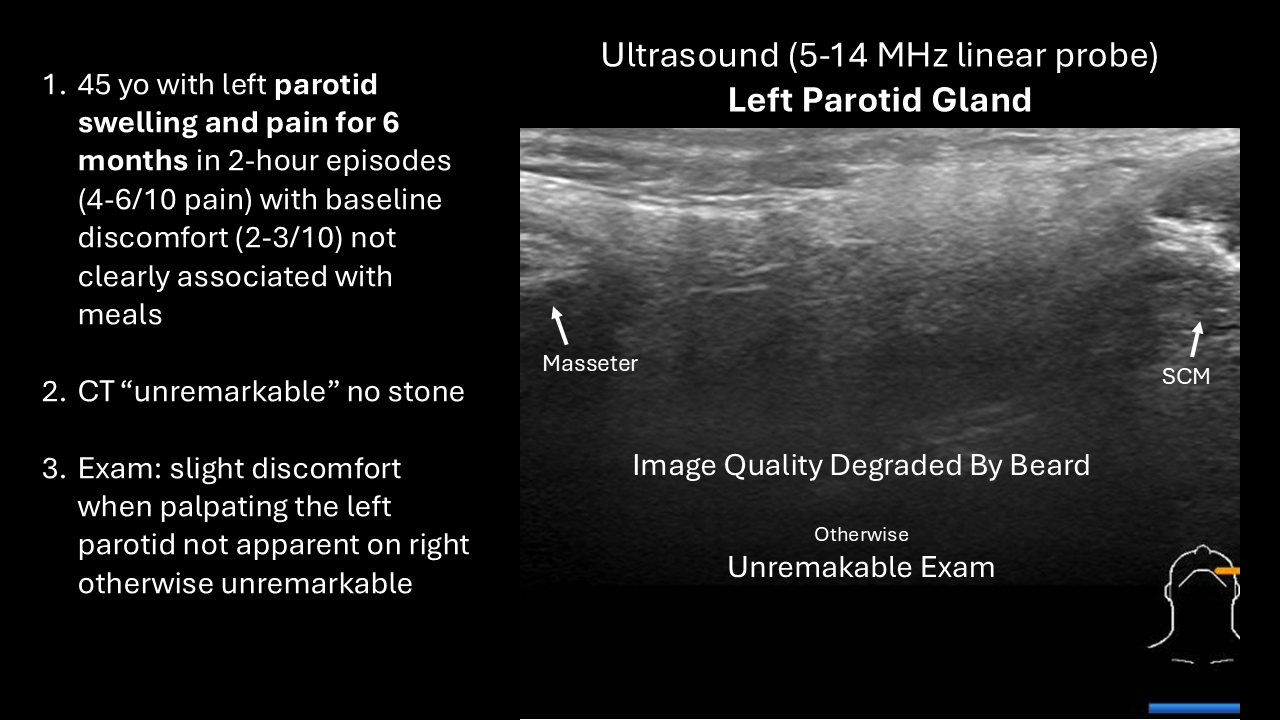
Case #5 Left Parotid Swelling and Pain
Presentation: 45 yo with left parotid swelling and pain beginning 6 months previously with episodes lasting 2 hours (4-6/10 pain) with baseline discomfort (2-3/10 pain) not clearly associated with meals.
Exam: clear saliva expressed from ducts of all four glands, left parotid slightly tender otherwise normal to palpation
CT: Unremarkable - no gland abnormality and no stone
Ultrasound (POCUS):
Panel Discussion Regarding Management
Outcome: Case #5 Left Parotid Swelling and Pain
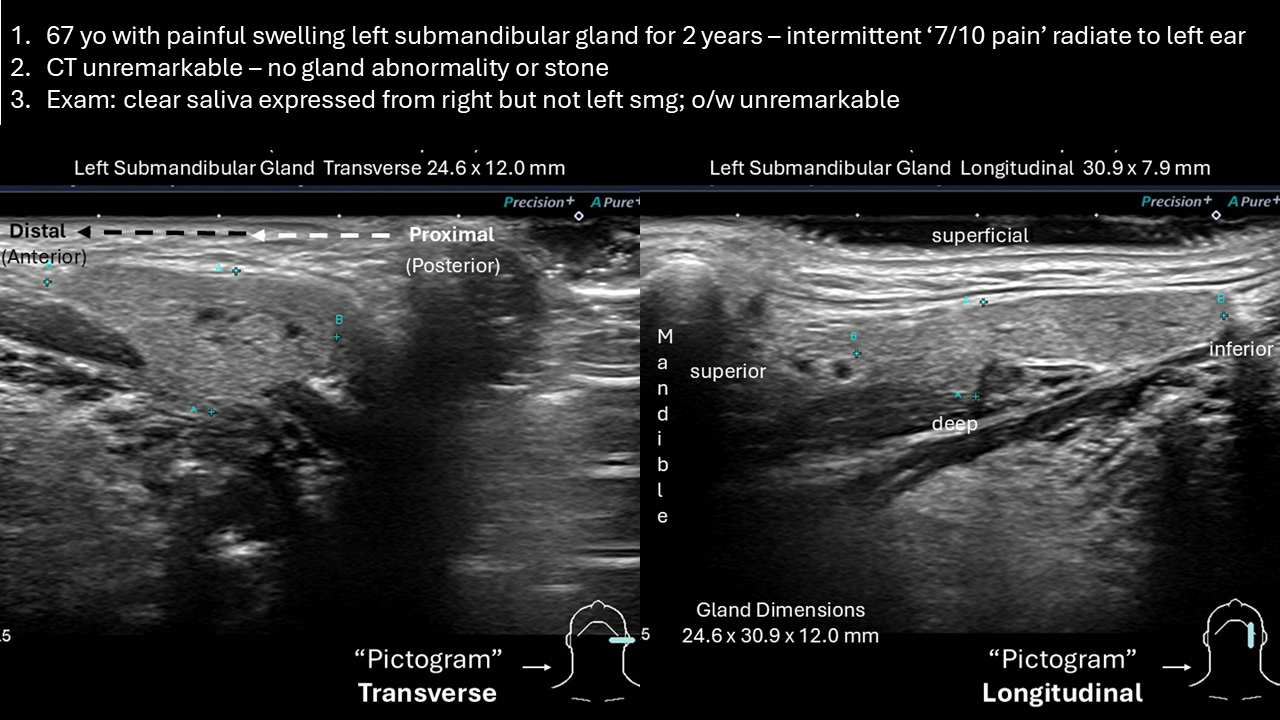
Case #6 Left Submandibular Pain With Swelling Unrelated to Meals
Presentation: 67 yo with painful swelling left submandibular gland preceding 2 years with intermittent pain "7 / 10" radiating to left ear
Exam: clear saliva expressed from right but not left smg; o/w unremarkable
CT: Unremarkable - no gland abnormality and no stone
Ultrasound (POCUS):
Panel Discussion Regarding Management
Outcome: Case #6 Left Submandibular Pain with Swelling Unrelated to Meals
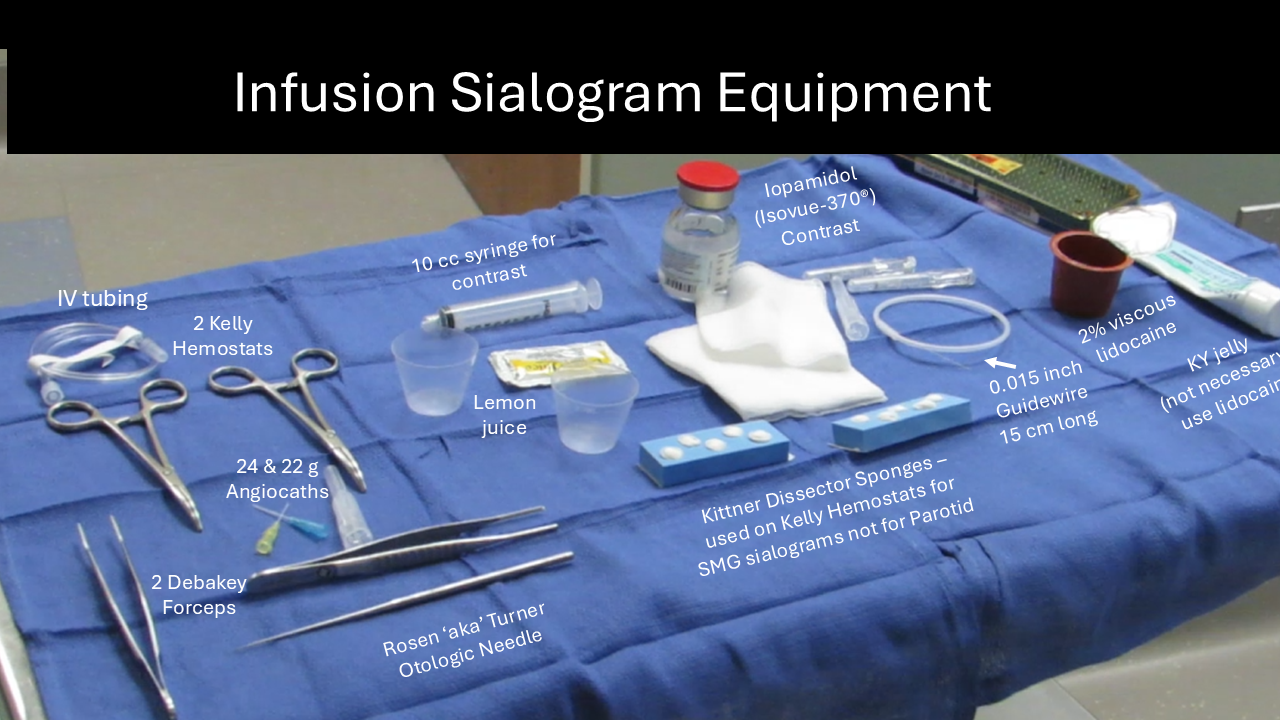
Equipment
Modified Procedure Note (for video above):
Procedure: Right parotid duct cannulation dilation with radiocontrast insufflation
Preop Diagnosis: Right parotid sialadenitis with likely sialolithiasis
Postop Diagnosis: Right parotid ductal strictures - stone not imaged
Anesthesia: Premedication with clindamycin, oral rinse with dilute Betadine, application of 2% viscous lidocaine to the right buccal area
Description of Procedure: Following identification the patient informed consent and a brief timeout in the fluoroscopy suite with her positioned supine the microscope was brought into identify an unremarkable right buccal region with a well identified parotid duct orifice into which a 0.015 inch guidewire was placed and then through a Seldinger technique a 22-gauge Angiocath placed over it and hubbed. Some slight backfilling was seen and then the hub was filled further with Isovue 370 allowing for performance of the sialogram as noted by radiology report below.
It is noteworthy that with the hub being of the 22-gauge it was initially directed into the accessory lobe hence the backfilling of saliva into the hub of the angiocath was only in the initial placement and not afterwards (see radiology report).
She tolerated the procedure well was examined in the otolaryngology clinic afterwards
Radiology Report
Procedure: FL SIALOGRAM COMPLETE
Indication: Sialadenitis, unspecified. 76 yo with h/o right parotid swelling, likely stone
Technique: Dr. Hoffman was present and performed cannulation of
the right parotid duct opening. After successful cannulation was
achieved, a 10-cc syringe with Isovue 370 contrast agent was
connected to the cannula and instilled into the duct under fluoroscopic
monitoring. A total of 2.5 cc of contrast agent was utilized. After
adequate duct opacification was achieved, AP and lateral spot
films were obtained. The cannula was then removed and duct was
allowed to empty following oral administration lemon juice to patient.
Post void AP image was then obtained.
Fluoro Time: 1:10
Radiation Dose: 326.4 uGy-m2 40.9 mGy
Findings:
Initial opacification was of the accessory gland. Catheter was
withdrawn slightly and adequate opacification of the parotid duct
and branches is achieved. There is distal salivary duct stricture
approximately 1 cm proximal to the papilla. Than there is a focal
area of significant ductal dilatation measuring approximately 6 mm.
The remainder of the main parotid duct shows irregularity with a
moderate to severe stricture in the midportion of the duct
(series 8, image 1) proximally 5 cm proximal to the papilla. Ductal
dilatation and irregularity extends proximally into the intraglandular
parotid ducts where they measure up to 3 mm. No definite
intraluminal filling defect is appreciated.
Post massage/lemon emptying film shows adequate emptying with no contrast remaining
within the gland or duct system.
Impression:
1. Significant parotid duct dilatation with prominent strictures
noted distally near the papilla and in the midportion of the main
parotid duct. Ductal irregularity and dilatation involves the
intraglandular ductal system as well.
2. No definite intraluminal filling defect to suggest stone is
appreciated.
The procedure and the results were discussed with the patient Dr.
Hoffman immediately following.
References:
Molotkova E, Wenzel P, Sylte J, Fain S, Maley J, Thorpe R, Hoffman H. Clinical Utility of Contemporary Digital Infusion Submandibular Sialography. Laryngoscope Investig Otolaryngol. 2025 Aug 21;10(4):e70248. doi: 10.1002/lio2.70248. PMID: 40852583; PMCID: PMC12369398.
Truong K, Hoffman HT, Policeni B, Maley J. Radiocontrast Dye Extravasation During Sialography. Ann Otol Rhinol Laryngol. 2018 Mar;127(3):192-199. doi: 10.1177/0003489417752711. Epub 2018 Jan 7. PMID: 29308655.
Wenzel PA, Thorpe RK, Maley JE, Policeni BA, Beichel RR, Henkle KD, Hoffman HT. Stensen's Duct Dynamic Anatomy Assessed with Sialography. Ear Nose Throat J. 2024 Aug 27:1455613241272451. doi: 10.1177/01455613241272451. Epub ahead of print. PMID: 39192625.
Foggia MJ, Peterson J, Maley J, Policeni B, Hoffman HT. Sialographic analysis of parotid ductal abnormalities associated with Sjogren's syndrome. Oral Dis. 2020 Jul;26(5):912-919. doi: 10.1111/odi.13298. Epub 2020 Mar 3. PMID: 32031309.
Thorpe RK, Foggia MJ, Marcus KS, Policeni B, Maley JE, Hoffman HT. Sialographic Analysis of Radioiodine-Associated Chronic Sialadenitis. Laryngoscope. 2021 May;131(5):E1450-E1456. doi: 10.1002/lary.29279. Epub 2020 Nov 17. PMID: 33200832; PMCID: PMC10049839.