return to: Sialography - How To and Do I Need To? Contemporary Infusion Digital Sialography
Presentation: 56 yo with 30+ yrs of xerostomia and xeropthalmia dx Sjogrens 15 yrs ago with +SSA +SSB. Has bilateral parotid swelling and pain every 4 weeks. Massage causes nasty taste in mouth
Exam: unremarkable (currently nontender) parotid glands with dry mouth unable to produce saliva with massage of glands
CT: atrophy of smg's; parotid glands with areas of fatty infiltration
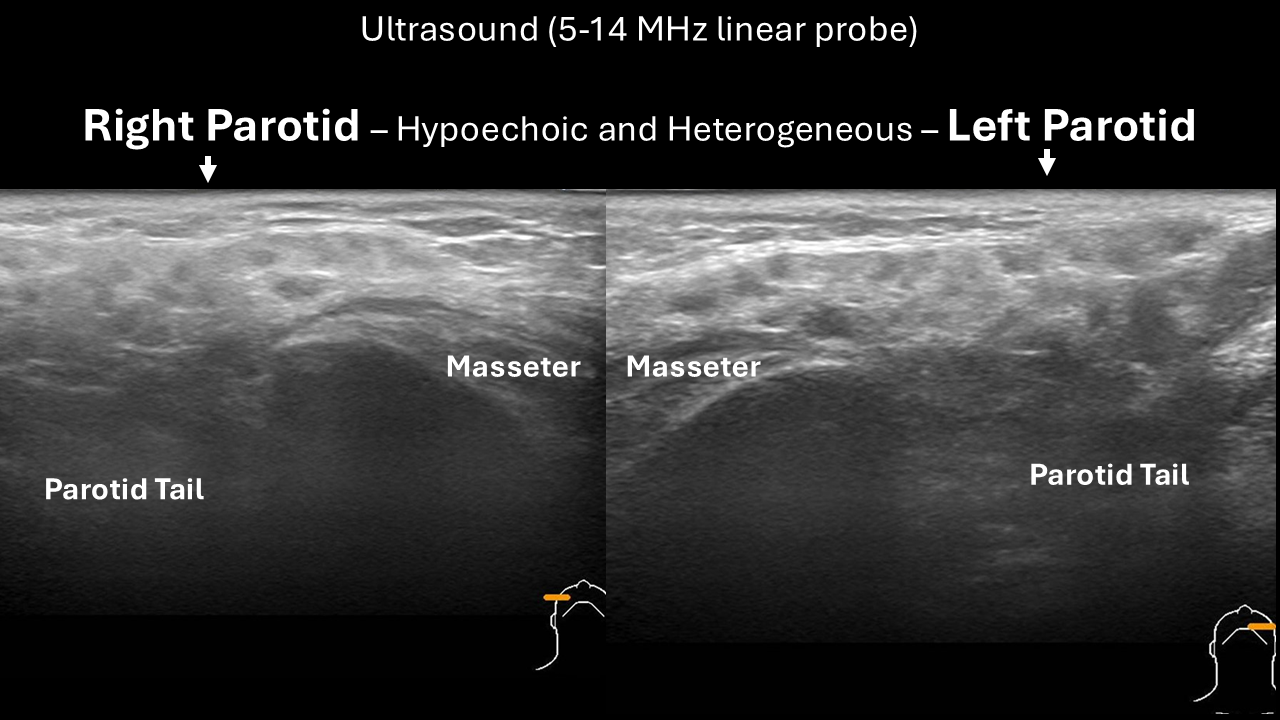
Ultrasound (POCUS at time of visit):
Panel Discussion Regarding Management
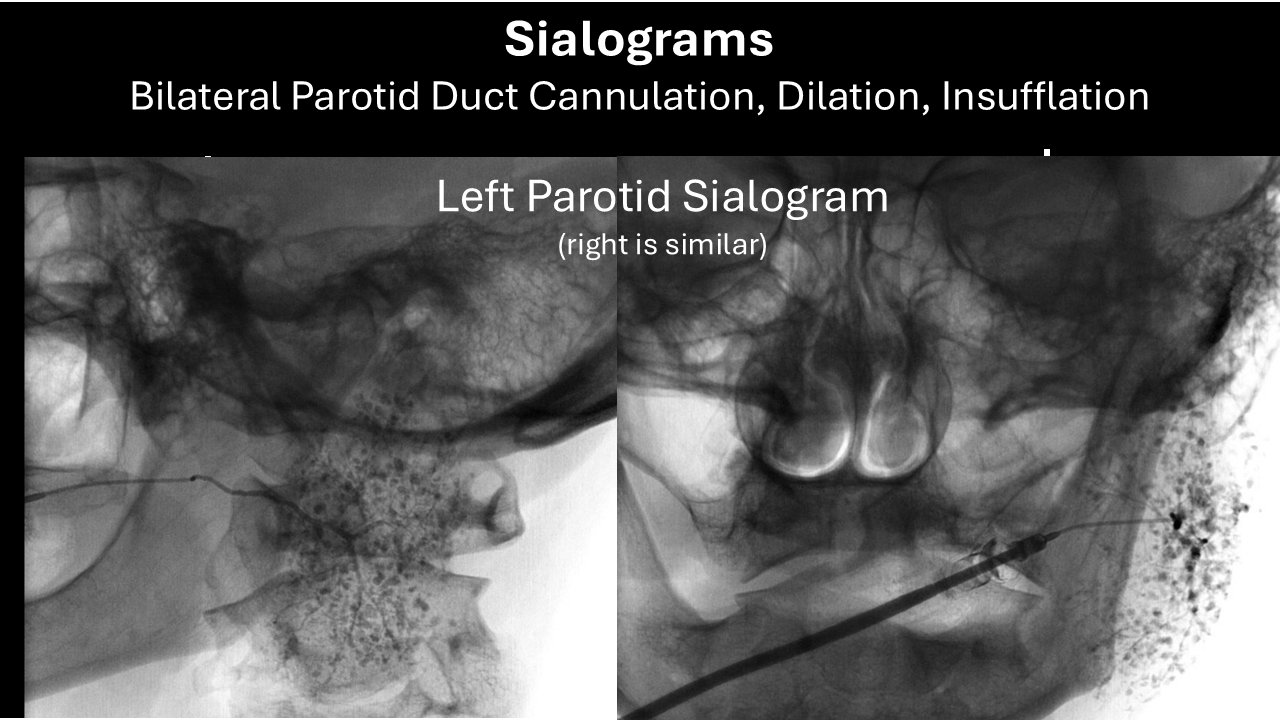
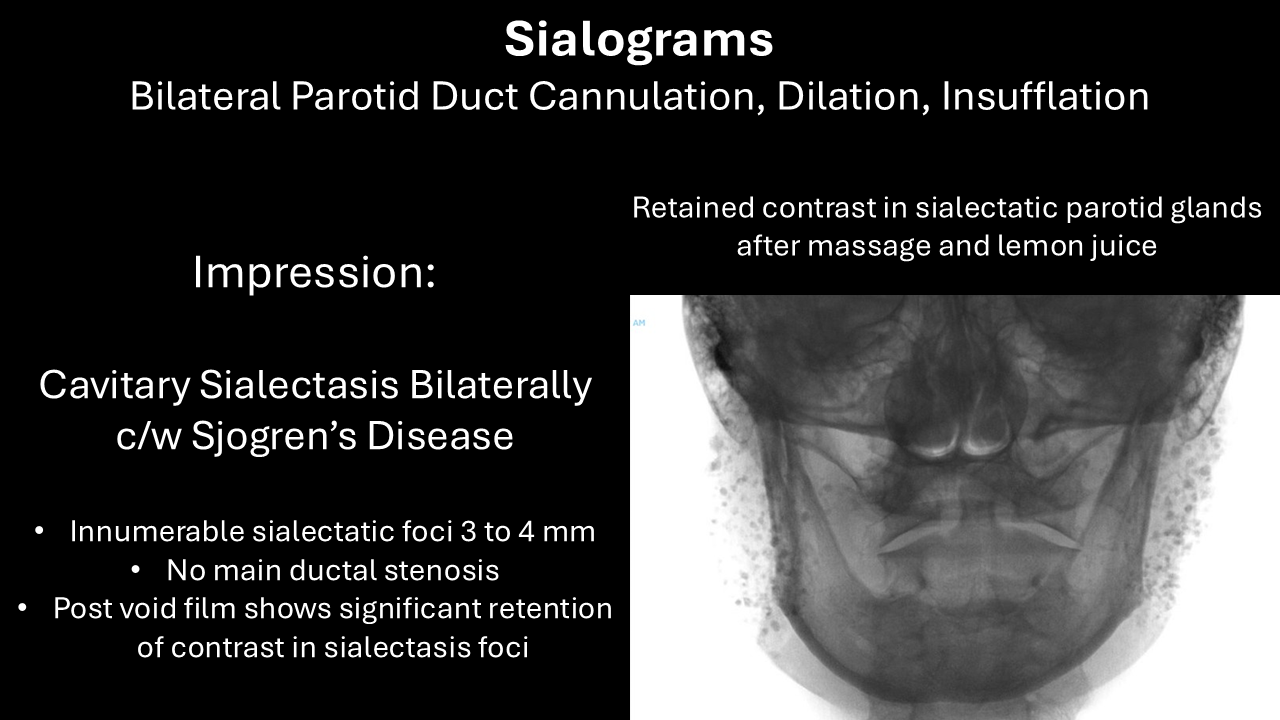
Sialograms:
Outcome:
- Immediately after sialogram in clinic: no tenderness or pain in either parotid - overall both feel better than before the sialogram
- 4 1/2 months after sialogram - marked improvement until symptoms beginning to recur past two weeks requesting steroid insufflation in clinic
- 6 months after sialogram In Clinic Procedure Bilateral Parotid Kenalog 10 Insufflation 10 months after sialogram - (see further below)
- 3 1/2 months after last steroid infusion one episode of swelling occurred prompting scheduling a future repeat steroid infusion.
Procedure Note
In-Clinic 6 months after sialogram
Bilateral parotid duct cannulation dilation with steroid (Kenalog 10) infusion (2.5 cc to each side with egress after infusion)
Preop Diagnosis: Sjogren's syndrome with sialadenitis–improvement following sialogram
Postop Diagnosis: Same
Anesthesia: Oral swab with Betadine to the buccal mucosa bilaterally, 2% viscous lidocaine applied topically to the buccal mucosa bilaterally, premedication with Augmentin begin the morning of the procedure
Description of Procedure: Following identification the patient informed consent and a brief timeout in the minor room bilateral parotid duct cannulation dilation with steroid (Kenalog 10) infusion
Following the above pretreatment ultrasound employing overhead illumination and loupe magnification with lateral traction on the left cheek the left parotid duct orifice was readily seen into which a 0.015 inch guidewire was readily placed followed by a 22-gauge angiocatheter through the Seldinger technique that was readily positioned followed by removal of the introducing 0.015 inch guidewire and application of a hemostat to the hub of the Angiocath allowing for placement of a Luer-Lok 5 cc syringe containing Kenalog 10 to be placed with gradual insufflation of the Kenalog allowing for hugging of the catheter with frequent interruptions to assess for patient comfort for the infusion.
An identical procedure was performed on the contralateral right side with the exception that the slower infusion done under direction by the resident was remarked upon by the patient as being less uncomfortable than the more rapid infusion I did on the left side. She tolerated both procedures well without significant discomfort reported and relates you felt pleased with leaving with identified fullness to both glands visibly by her report palpably it also by ultrasound then repeated showing infusion to bptj parotid glands perfusing the parenchyma well