See also: Anterior Cervical Fusion and Vocal Cord Paralysis
Case History
The patient reviewed for this case has a history of C5-T1 anterior cervical discectomy and fusion (ACDF), with evidence of hardware failure on the caudal end of the fusion. The patient also has a prior medical history significant for a thyroidectomy, and so hardware revision was pursued through a transcervical approach, with neurosurgery as the primary team and otolaryngology assisting in the surgery to aide in minimizing risk of vocal cord injury or paralysis. Prior to the procedure, the patient had no noticed changes in her voice or other neurologic deficits.
Consent
Risks, benefits, and altenatives to the procedure are to be discussed with the patient. The risks include but are not limited to infection, bleeding, muscle weakness, and damange to the vocal cord(s). The possible impact on speech and voice function is to be discussed with the patient should should damage to the vocal cord occur.
Procedure
Cervical spinal fusion through an anterior transcervical approach.
Procedure Note
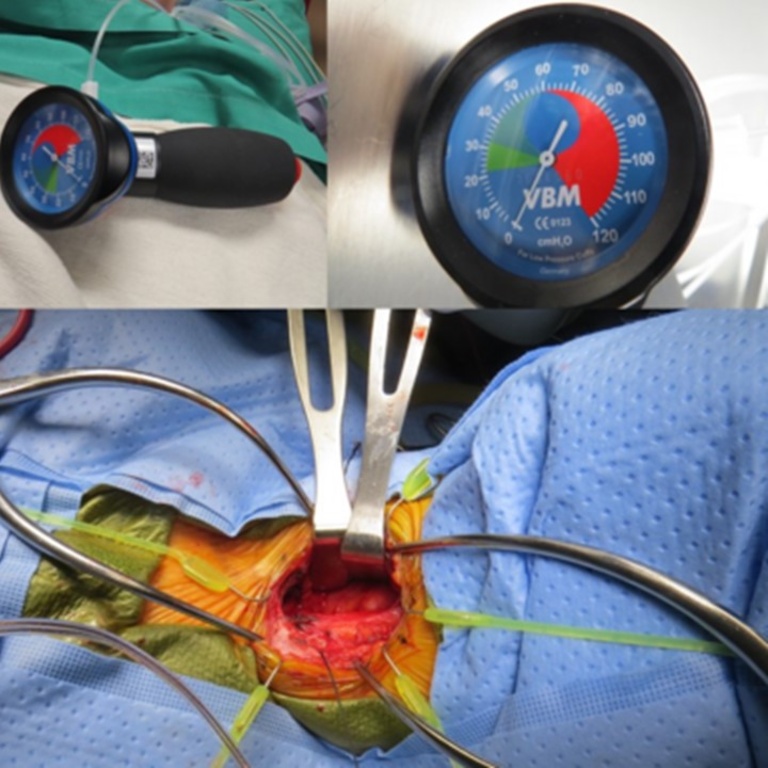
The patient was induced and intubated by anesthesia with a 6-0 MLT ETT with cuff pressure measured at 10 mmHg. A solution of 0.5% lidocaine with 1:200,000 epinephrine was first injected into the previous ACDF incision. A skin incision was performed by the neurosurgery team at the prior incision site, with subsequent dissection deep into the tissue along the scar tract until the medial visceral compartment and lateral carotid sheath were encountered. The otolaryngology team then continued the dissection, medializing the visceral compartment and continuing dissection deeply with lateralization of the carotid sheath with Kittners until the previous ACDF plate and screws were clearly encountered over C5-T1. Following adequate retraction, the endotracheal tube cuff was deflated, repositioned, and reinflated to an appropriate pressure. The case was then turned back over to neurosurgery for the completion of the ACDF revision. This concluded the Otolaryngology portion of the procedure. The neurosurgery team then completed the remainder of the C5-T1 ACDF revision, which the patient tolerated well.
Risk of Vocal Cord Paralysis
One of the risks associated with an anterior cervical approach surgery, such as ACDF, is a risk of damage to the recurrent laryngeal nerve resulting in vocal cord paralysis. The estimated incidence of such damange varies in the literature, however the incidence has been reported to be as high as 22%. Erwood et. al utilized a convenience sample of sequential patients requiring reoperative ACDF, totalling a sample of sixty-seven patients, and noted that five patients had new onset vocal cord paralysis post-operatively.1 However, each of these cases had resolved symptoms within 2 months after the operation. However, there are other case reports of bilateral vocal cord paralysis occuring following ACDF, suggesting that there a significant incidence of this complication.2,3 Further research is needed to better characterize the rate of this complication, and to better identify how many patients experience lasting deficits following surgery.
Given the concern for this complication, there has been investigation to identify methods to prevent it. However, the exact mechanism(s) behind the occurence of vocal cord paralysis is not well characterized, however it is likely due to injury to the recurrent laryngeal nerve. One such mechanism of injury is the compression of the recurrent laryngeal nerve due to increased pressure in the endotracheal tube cuff. During exposure of the surgical field, retraction is used to manipulate and pull the soft tissues of the anterior neck. However, during this process it is believed that the force of the retractors could be applying an external force onto the larynx and the endotracheal tube cuff, resulting in an increased effective pressure in the cuff. As such, Apfelbaum et. al conducted a study using a sample of 900 patients (650 of whom underwent the intervention) who underwent anterior cervical spinal surgery.4 The intervention used was to deflate the endotracheal tube cuff after retractors had been placed, repositioning the endotracheal tube as needed, and reinflating the endotracheal tube cuff to an appropriate pressure. In the intervention group, the rate of temporary paralysis of the vocal cords decreased from 6.4% to 1.69% (P = 0.0002), suggesting that pressure from retraction and the endotracheal tube cuff has a role in compression injury of the recurrent laryngeal nerve.
Given concern for pressure injury of the recurrent laryngeal nerve during ACDF surgery, a consideration during surgery is to readjust the pressure in the endotracheal tube cuff once adequate retraction has been established, and to reposition the endotracheal tube as needed. However, further research should still be done to better characterize this method of vocal cord injury, as well as to better identify true risk and long-term complications of vocal cord injury following ACDF surgery.
References
1. Erwood, M. S., Walters, B. C., Connolly, T. M., Gordon, A. S., Carroll, W. R., Agee, B. S., Carn, B. R., & Hadley, M. N. (2018). Voice and swallowing outcomes following reoperative anterior cervical discectomy and fusion with a 2-team surgical approach, Journal of Neurosurgery: Spine SPI, 28(2), 140-148.
2. Jacobson L. Bilateral vocal cord paralysis. Bilateral vocal cord paralysis following anterior cervical fusion. Anaesthesia. 1979 Nov-Dec;34(10):1020-3. doi: 10.1111/j.1365-2044.1979.tb06251.x. PMID: 539637.
3. Manski TJ, Wood MD, Dunsker SB. Bilateral vocal cord paralysis following anterior cervical discectomy and fusion. Case report. J Neurosurg. 1998 Nov;89(5):839-43. doi: 10.3171/jns.1998.89.5.0839. PMID: 9817425.
4. Apfelbaum, Ronald I. MD; Kriskovich, Mark D. MD; Haller, Jeffrey R. MD. On the Incidence, Cause, and Prevention of Recurrent Laryngeal Nerve Palsies During Anterior Cervical Spine Surgery, Spine: November 15, 2000 - Volume 25 - Issue 22 - p 2906-2912
