return to: Sialography - How To and Do I Need To? Contemporary Infusion Digital Sialography
Case #2
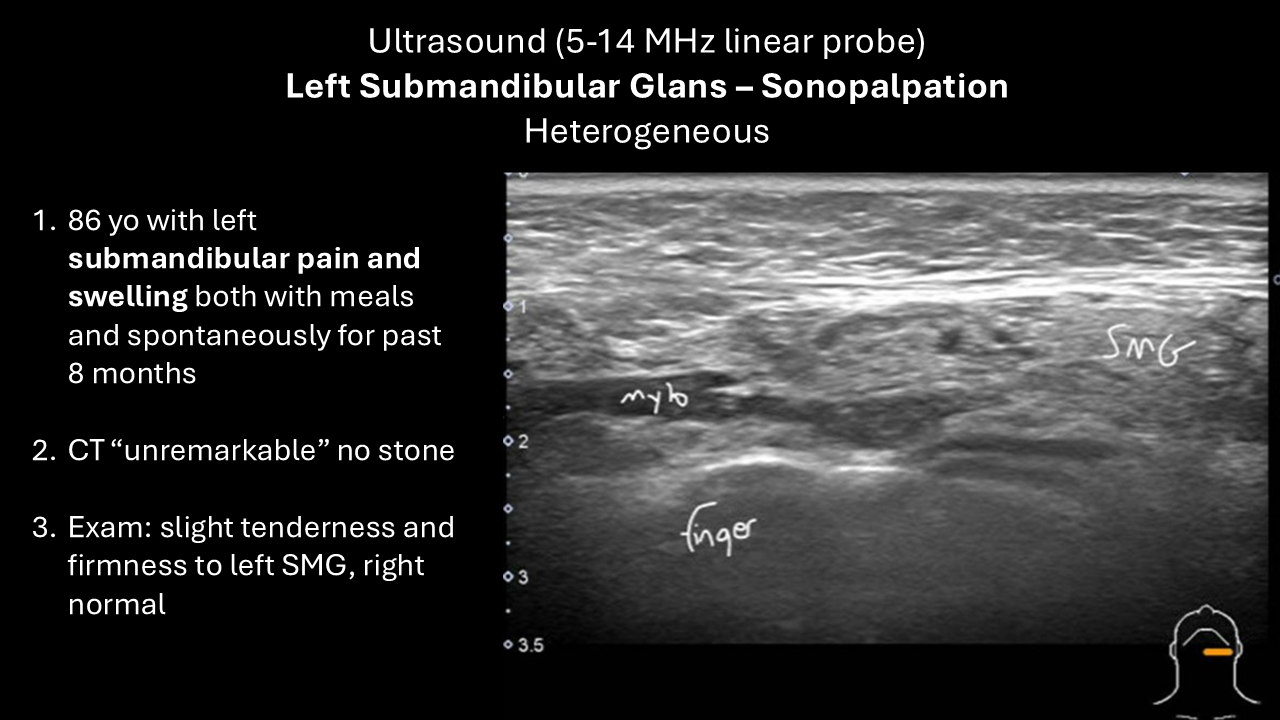
Presentation: 86 yo with left submandibular pain and swelling both with meals and spontaneously over 8 months.
Exam: slight tenderness and firmness to left submandibular gland, right is normal
CT: unremarkable salivary glands - no stone
Ultrasound (POCUS at time of visit):
Panel Discussion Regarding Management
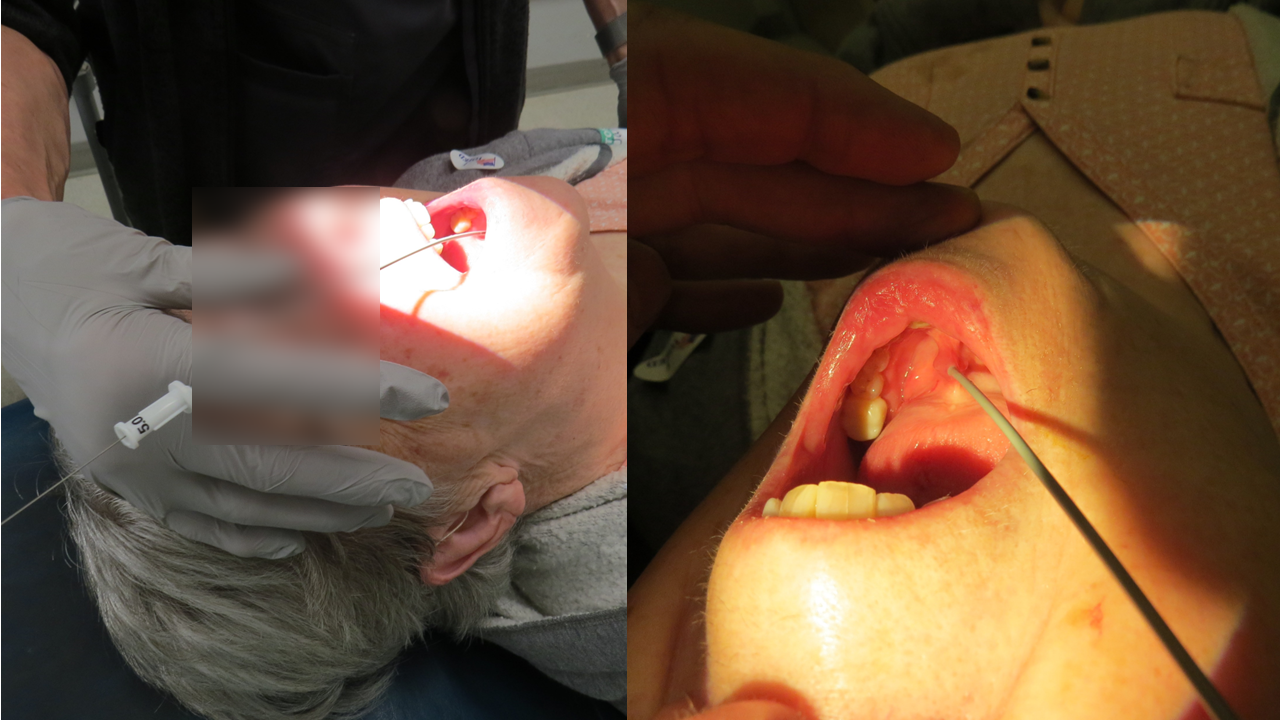
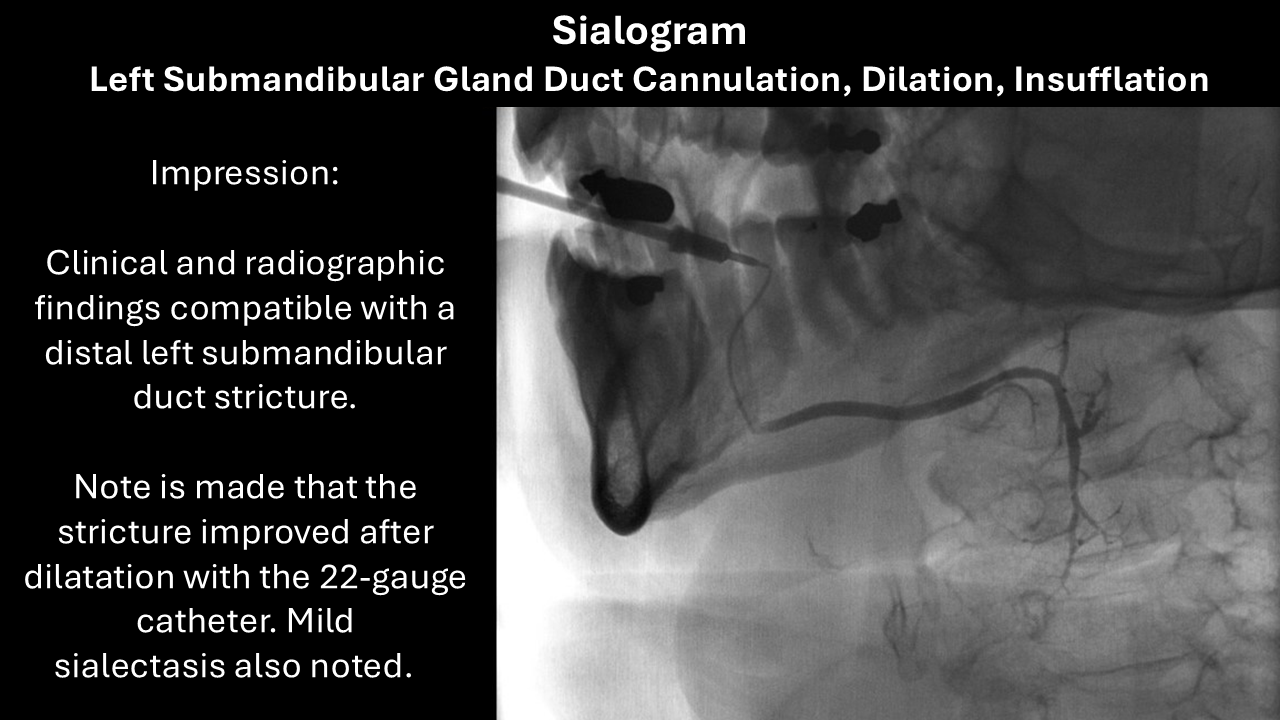
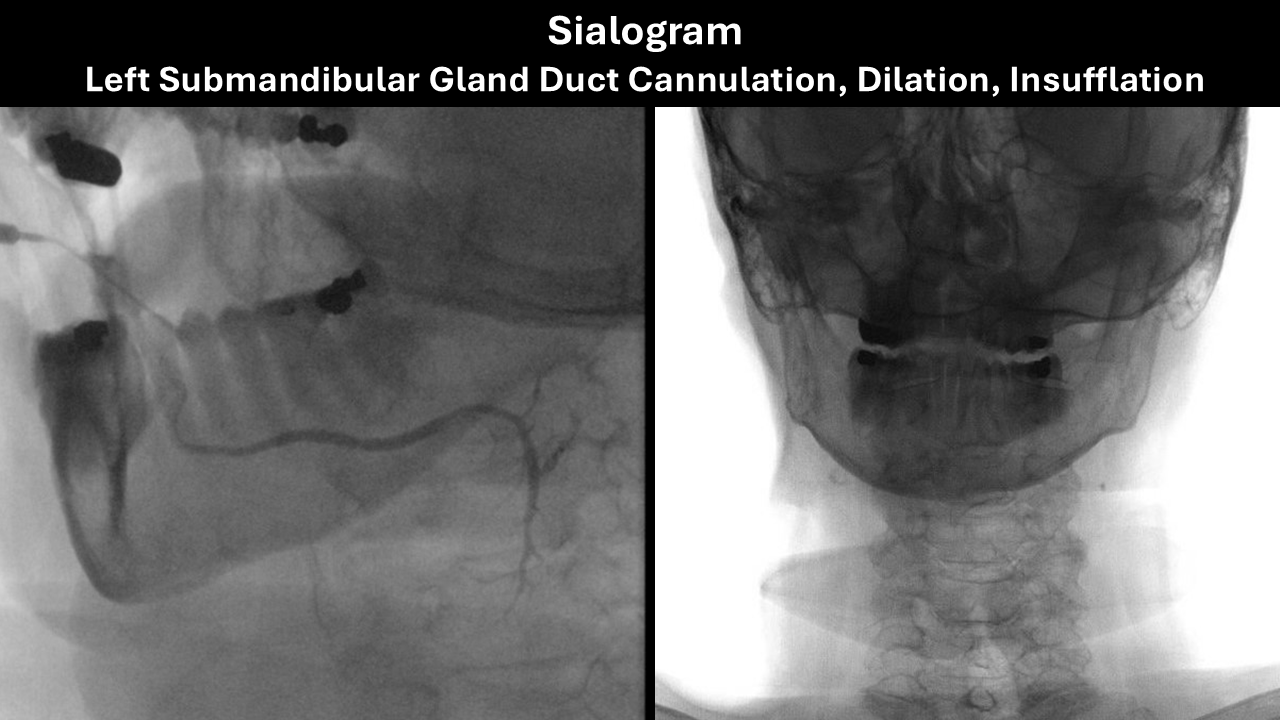
Sialogram:
Outcome:
- Immediately after sialogram in clinic: "this was now the best her left submandibular gland had felt in 2 years". Exam: Successful massage of the gland with the duct showing clear material (saliva vs Isovue®) emanating from it. We suggested maintenance of good hydration and massage would be helpful to hopefully prevent recurrence with the understanding which were she to have recurrence more aggressive dilation could be done possibly in the clinic
- Symptom Free for 9 months then recurrence of symptoms
- In Clinic Procedure Duct Dilation 10 months after sialogram - (see further below)
- Symptom Free at Last Follow-up (10 months after in clinic dilation; 20 months after sialogram)
Procedure Note
In-Clinic Dilation 10 months after sialogram)
Left submandibular duct cannulation dilation with Kenalog® 10 diluted with lidocaine insufflation (2.5 cc of "Kenalog® 10" created by mixing Kenalog 40 part with 3 parts of 1% lidocaine)
Preop Diagnosis: Left submandibular sialoadenitis with ductal narrowing previously responsive to a sialogram
Postop Diagnosis: Same
Anesthesia: Premedication with antibiotics as well as oral application of 2% viscous lidocaine and Betadine swab to the floor the mouth
Description of Procedure: Following identification the patient informed consent and a brief timeout in clinic room B1 with her placed in the semi recumbent fashion with the microscope brought in from above initial difficulty in identifying the left submandibular duct orifice was facilitated by massage of the right showing equivalent area in the left and then massage allowing for placement of a Rosen needle (Turner needle) followed by manipulations requiring 2 DeBakey forceps to straighten the duct allowing for cannulation with a 0.015 inch guidewire 15 cm long over which is progressive dilation with a 24 and then a 22-gauge Angiocath was performed.
With a 22-gauge angiocath in place the guidewire was removed and the "Kenalog 10®" ["Kenalog 10®" = one part Kenalog 40®, three parts 1% lidocaine] preparation was instilled to a volume of 2.5 cc with her affirmation the pain was similar to that which she has had with eating but a lesser extent and after the initial pain on insufflation had no further pain and actually even relief of the pain from that which she came in with
Through the 22-gauge Angiocath in place a 30 cm long 0.015-inch guidewire was placed with removal of the 22-gauge Angiocath and then used successively of a 5 and 6 then final 7 French Cook salivary access dilator placed to a depth of approximately 3 cm successfully left in place for 2 minutes for the 5 and 1 minute for the 7
She tolerated the procedure well with no pain inspection of the area and photographs taken during the course of the procedure